

Breathing is one of the most important functions of the vital activity of human body. Lack of breath for several minutes leads to the death of a body. Breathing is accompanied by a number of physical, biochemical and nervous processes, the disturbances of which lead to pathologies of the respiratory function as a whole. Breathing provides oxygen gas exchange to carbon dioxide and the removal of water from a body. In the process of breathing, several structural units of the body participate, each of which performs its function and, in turn, has a rather complex organization. The main ones are the nose with the paranasal sinuses and the lungs. The nose of the paranasal sinuses protects the human body from the influence of harmful factors in the air environment. Lungs provide the main function of breathing - gas exchange. In addition, the breathing is affected by a condition of the nasopharynx and the trachea.One of the most common pathologies of breathing is snoring during sleep. Snoring is primary, does not lead to a breakdown in the structure of sleep and is not accompanied by negative consequences.
The major danger is snoring as a sign of obstructive sleep apnea (OSA), when breathing stops repeatedly during sleep. Apnea several times increases the risk of cardiovascular disease, heart attack and stroke, causes daytime drowsiness, shortness of breath and other unpleasant symptoms.
Despite the danger of OCA, there are no clear diagnostic indicators for its diagnosis and effective
treatment methods. Use manual and instrumental methods for diagnosis of OCA.
Manual methods determine the following indicators:
A video recording of sleep can provide additional information.
Simultaneous registration of all indicators, their ranking and decision making is an extremely ambiguous task. Final diagnosis is the result of simultaneous consideration of a large set of quantitative and qualitative indicators of a patient. Final diagnosis is the result of information received by a doctor, doctor makes the final decision on the basis of information received and in each case tries to recognize or recall what he met in his practice. There is a transition from abstract to specific diagnosis, taking into account all the characteristics of a patient. From the point of view of psychology, this is the receipt of new information, creativity or productive thinking.
To reduce the subjective factor in the formation of a diagnosis, artificial intelligence should be used. At first glance, the means of artificial intelligence would have to replace a person in making decisions. However, with respect to medicine, especially to our task.
there are several insurmountable obstacles:
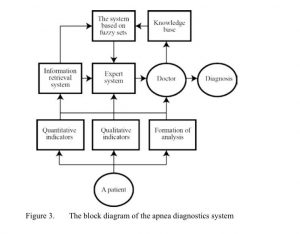
Feature of the diagnosis of OSA is the availability of a large number of qualitative (linguistic) and quantitative indicators. For the analysis of associations with linguistic indicators, information retrieval systems (IPS) are traditionally used. Quantitative indicators can serve as the basis for an expert system (ES). Taking into account the peculiarities and difficulties of diagnosing OSA, the structure of the biotechnical diagnostic system was developed, the feature of which is the fact that the doctor is an integral part of the diagnostics subject, along with technical means. (Figure 1)
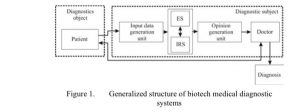
In given structure of the system, three blocks of information transformation can be distinguished: the block for generating input data; block formation of the conclusion and an information processing unit consisting of the synthesis of expert and information retrieval systems. The coordinated work of all the units should ensure a qualitative medical diagnosis, taking into account the knowledge of the doctor.
An objective diagnosis is possible in the event of the greatest possible increase in the capabilities of all components of the system. In practice, the capabilities of the components of the system can be increased to certain limits.
Increase the capabilities of each component of the system will be analyzed in their relationship and the assumption of maximum adaptation of the technical and biological links of the system. The main task of adaptation is to maximize the use of technical means and stimulate the thinking of the doctor.
At first stage of the design of the apnea diagnostic system, the question of linguistic indicators ranking was considered. The definition of numerical correspondences of qualitative indicators (scaling) implies the ranking of such concepts as "always - often - sometimes - rarely - never". It is necessary to justify the following:
I = Plog2 1 + (1−P)log2 1 , (1)
P 1−P
where I is informativeness, directly related to the linguistic variable. By formula (1) (Figure 2), it is possible to determine numerical values of variables, in this case probabilities.
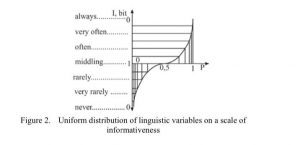
Using formula (1), we obtain the distribution of linguistic variables according to the scale of probabilities, taking into account the informativity (Figure 2). Thus, we take into account the peculiarity of medicine, where, in addition to probability, the informative value of the indicator is of great importance.
An important and ambiguous task is to choose the number of qualitative variables. The upper limit of the number of variables is 11-13. On the other hand, the minimum number of variables in determining the degree of belonging to the indicator must contain at least two values (0 and 1, respectively) [3].
The third mandatory point should be the middle of the scale - 0.5. The remaining points are between 0 and 0.5 (and a symmetrical interval of 0.5 ... 1) and their number can vary from 0 to 4 (with 11 divisions).
In medical diagnosis, a fourth mandatory point may appear, which lies outside the scale. This point - the linguistic variable "unknown", "no information" covers the entire scale. In our case, to evaluate linguistic indicators, we select a three-level scale.
After choosing the method of accounting for medical knowledge and data, consider the question of methods of processing information.
The most time consuming part of creating an IPS is the formation of a matrix of the associativity of terms, on which the completeness of the information provided on request depends. At the heart of most associative indexing methods lies the matrix of the associativity of terms, which assigns for each pair of terms a corresponding indicator of associativity.
The principle of its use is as follows: if q is an ordinary vector of terms (for example, a query vector), then one can obtain an extended vector q 'with the help of a vector equation:
R*q = q` (2) where R is the matrix of terms association; q is the vector of the request. q` is an extended query vector that takes into account the additional terminology relations specified in R. We will use the matrix of terms association in the interpretation of the model, according to which:
the weight value of a word, regardless of its presence in the original, increases in the case of words existence associated with it in the dictionary sample of the array.
the weight value of a word having a relatively insignificant informative value is reduced, due to the presence of a connection with words that have little informative value.
document normalized in relation to the size of the document:
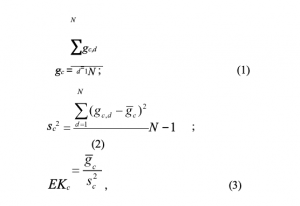
where N is the number of documents in the sample; gc,d = fc,d/Ld is the normalized frequency of occurrence of the word c in the document; fc,d is the number of occurrences of the word c in document d; Ld - the number of words in the text taken (truncated words in document d).
The coefficient of pairwise connectedness F is calculated from the next considerations. For a set of n documents, the typical indicator of the associativity (pairwise connectedness) of terms i and j can be simply the sum of products of the corresponding frequency terms:
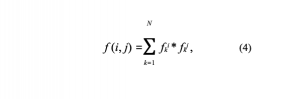
summation is made for all documents. In addition, associativity indicators could be normalized to obtain a certain coefficient ranging from 0 for completely unrelated pairs to 1 for fully associated pairs. The normalized coefficient of associativity is the coefficient:
Implementation of the actual network model:
j:i≠ j where I is the query matrix equivalent to the matrix of given currents; E is an index matrix equivalent to the matrix of induced stresses; C-1 - matrix of terms association, obtained by inversion of the matrix C, compiled by the expert; cij is the element of the matrix C; fijis the associativity coefficient of the terms i and j.
IPS provides the formation of a preliminary detention and significantly reduces the time the decision is made by a doctor.
No less important task of creating a system for diagnosing OSA is the creation of a subsystem for forming a conclusion. Medical diagnostics are traditionally attributed to one of the areas where it is very difficult to apply the exact formal methods of decisionmaking. However, in recent years, more and more talk about the transition to evidence-based medicine. The aspiration to satisfy the criteria of "evidence" maximally leads to the need for deep formalization of the subject area, as the basis for creating reproducible decision algorithms. On the other hand, formalization leads to the formation of a field of knowledge containing thousands, and even tens, hundreds of thousands of elementary concepts and processes - investigative, associative and other connections [7].
In AI theory, the main goal is to learn how to store and process information like human intelligence. With the development of AI, most of the knowledge has been concentrated in data structures (tables, lists, abstract data types), that is, the role of declarative knowledge increases. In most existing AI systems, knowledge is considered to be sentences written in knowledge representation languages that are close to natural language.
Our system based on the principle of linguistic input and output information. In accordance with this principle, the inputs of an object and its output are considered as linguistic variables that are evaluated by qualitative terms.
The principle of forming the structure of "inputoutput" dependence in the form of a fuzzy knowledge base. Fuzzy knowledge base is a set of rules IF (inputs), TO (exit), which reflect the expert's experience and his understanding of cause-effect relations in the considered decision-making problem. The peculiarity of such statements is that their adequacy does not change with insignificant fluctuations in the experimental conditions. Therefore, the formation of a fuzzy knowledge base can be considered as an analog of the stage of structural identification, on which a rough model of the object with parameters to be adjusted is built. In this case, the forms of the fuzzy terms membership functions are used to estimate the inputs and outputs of the object.
To configure the expert system on the basis of fuzzy logic, a software product (Fuzzy) is used to collect, store and use the knowledge obtained from experts to solve applied problems of identification and decision making, as well as a software environment that allows creating expert systems in the chosen subject area. The membership functions will be based on the statistical processing of the opinions of the expert group. Each expert fills in a questionnaire, in which the opinion is indicated, about the presence of fuzzyui = (i =1,n) set elements. ~lj = ( j =1,m)
We introduce the next notation: K - the number of experts, opinion of the k-th expert on the presence of the ui element of the properties of a fuzzy set ~lj , k=1,K , i =1,n, j =1,m. We assume that the expert estimates are binary bkj,i ∈{0;1} , where 1 indicates the presence of ui properties of fuzzy sets ~lj , and 0 - in their absence.
Based on the results of the questionnaire, the degree of belonging to the fuzzy set is calculated as follows:
It is assumed that membership functions will be built for the three terms "low", "medium", "high", used to assess linguistic indicators. The results of processing the opinions of experts allow us to construct the functions of belonging to the fuzzy set of the corresponding element. The use of this approach makes it possible to evaluate quantitative and qualitative indicators on a unified scale. In addition, the proposed system uses the capabilities of information qualitative indicators on a unified scale. In addition, the proposed system uses the capabilities of information retrieval and expert systems, which to some extent imitate the decision-making process of a doctor.
The scheme of the developed system for the diagnosis of apnea is shown in Figure 3.
Snoring is one of the signs of obstructive obstructive sleep apnea - a disease that is difficult to diagnose and treat.
The basis for the diagnosis of apnea is a set of noncorrelating qualitative and quantitative indicators.
The structure of the biotechnical diagnostic system of apnea is proposed. This feature is the joint work of technical means of registration, information processing and a doctor.
To implement the system, the method for estimating qualitative indicators and the principle of creating an information retrieval subsystem are justified.
It is proposed to use neural network technologies and the theory of fuzzy sets to create an expert subsystem.